—Garrett lives with severe hemophilia A


WHEN IS IT TIME
TO TURN THE TIDE?
Each day, living with hemophilia may feel like riding a wave of uncertainty. Managing your hemophilia can be demanding. But the landscape is changing. Learn more today.
We are Novo Nordisk, a company committed to advancing research in hemophilia.
Garrett has severe
hemophilia A.
WHEN IS IT TIME
TO TURN THE TIDE?
Each day, living with hemophilia may feel like riding a wave of uncertainty. Managing your hemophilia can be demanding. But the landscape is changing. Learn more today.
We are Novo Nordisk, a company committed to advancing research in hemophilia.
How do you feel about your ability to prevent bleeds and manage your hemophilia?
"The bleeding, bruising, and 3 IV infusions per week were not the greatest challenges of hemophilia. It was feeling abnormal, fearing that others would treat me differently, and coping with my seemingly unfair reality."

A 2023 survey showed people with hemophilia continued to experience physical and mental burden.a
In a recent survey of 472 people with hemophilia currently on treatment, many respondents said they suffered physical and mental burden regardless of the treatment they were taking. How do the results of the survey compare with your experience?
People who have hemophilia reported feeling anxious and worried about bleed protection:

Feeling anxious that their current treatment did not provide adequate bleed protection at least sometimes (N=113)b

Feeling worried that their current prophylactic treatment did not provide adequate bleed protection at least sometimes (N=101)b
aData Source: PicnicHealth.
bQuestions asked were: “How often do you feel anxious that your current treatment might not be adequately protecting you from bleeding?” and “How often do you feel worried that your prophylaxis treatment does not adequately protect you from bleeding?” Response options were “Never,” “Rarely,” “Sometimes,” “Often,” and “Always.” N data represents the number of respondents that answered sometimes/somewhat or higher to each question.
People with hemophilia also reported administration difficultiesc:

were at least somewhat
bothered by:
“the need to carry my medication when I am out” (N=84)

experienced at least some difficulty:
“putting the needle correctly in my body” (N=35)

found it at least somewhat difficult:
“finding a good place on my body to inject” (N=53)

of people with hemophilia reported that they postpone, delay, or miss a treatment on purpose at least sometimes (N=87)
cPeople with hemophilia responded to questions from the Hemo-TEM questionnaire on a 5-point scale: not at all/never, a little/rarely, somewhat/sometimes, very/often, or extremely/always.
People with hemophilia reported the aspects of treatment that bothered themc:
29%
needing to carry medication and supplies when out (N=84)
24%
having to find time in schedule for treatment (N=72)
25%
how often they need to give themselves treatment (N=75)
19%
how long it takes to prepare and give treatment (N=57)
25%
needing to store medication and supplies
(N=73)
20%
the number of steps it takes to give treatment (N=61)
People with hemophilia reported that scarring, bruising, and pain were among the most common physical administration burdens they experiencedc:

People with hemophilia reported ongoing emotional burdenc:

People with hemophilia reported disruption in daily activitiesc:
Results showed disruptions to day-to-day activities, such as work or school, and interference with social events and vacations.
Garrett has severe
hemophilia A.


Percentage of survey respondents who reported that current treatment interfered with daily activities:

(N=42)
reported that their treatment interfered
“with work or school at least somewhat”
(N=69)
reported that their treatment interfered
“with travel or vacations at least somewhat”

(N=44)
reported that their treatment interfered
“with social activities at least somewhat”
People with hemophilia still experience bleedsd:
Hemophilia A without
Inhibitors

Bleeds per year
N=308
Hemophilia A with
Inhibitors

Bleeds per year
N=23
Hemophilia B without
Inhibitors

Bleeds per year
N=95
Hemophilia B with
Inhibitors

Bleeds per year
N=7
dMean annual bleed rates (ABRs) were calculated from EMRs of the broader population (N=472) for generalizability.
Educational resources built for you
Our Hemophilia Dictionary defines common terms and concepts to make it easier to talk about and understand various bleeding disorders.
Are you interested in learning about research in hemophilia?
Learn about different approaches being researched to manage hemophilia.
Different approaches to hemophilia management are currently being researched.
Let’s explore different approaches that aim to restore balance between bleeding and clotting.
When a blood vessel becomes injured, a series of steps take place to form a clot and prevent bleeding. This is called the coagulation cascade, also known as the clotting cascade. It involves a balance between clotting proteins and anticoagulant proteins.

People with hemophilia A do not produce enough of the clotting protein Factor 8, and people with hemophilia B do not produce enough of the clotting protein Factor 9. This results in the inability to form clots properly and puts people at risk of bleeding.
Different approaches are being researched that do not replace missing factor, but instead target different parts of the coagulation cascade that aim to improve clot formation.
- These approaches are also looking at ways to address challenges of some current hemophilia treatments through different forms of administration.
A different approach aims to restore balance in the clotting cascade by blocking anticoagulant proteins rather than replacing clotting factors.
The goal is to restore balance between bleeding and clotting without the need for replacement factor.
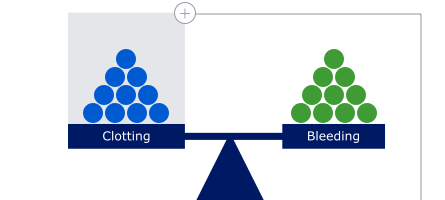
People without hemophilia
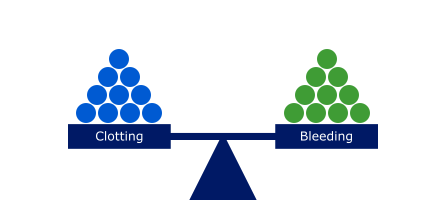
In people without hemophilia, there is a balance between bleeding and clotting and the ability for blood to coagulate when needed.
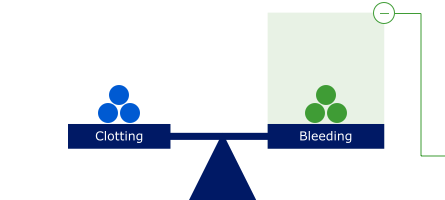
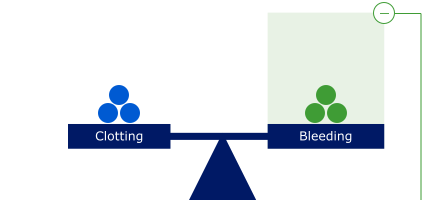
People with hemophilia
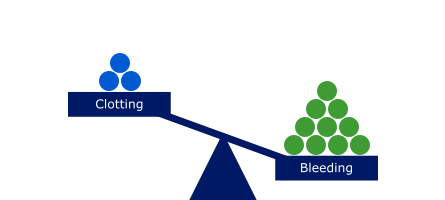
In people with hemophilia, there is a lack of clotting Factor 8 or Factor 9, disrupting the balance between bleeding and clotting. This results in a bleeding tendency because the blood is unable to clot when needed.
Factor replacement
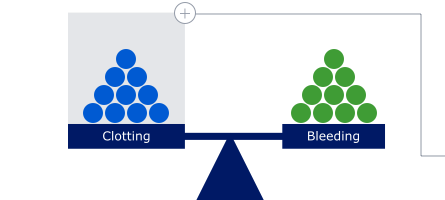
Treatment classes that increase clotting proteins:
Factor 8 or Factor 9 | Bypassing agents | Factor 8 mimetic | Gene therapy.
Factor replacement therapies restore balance by adding more clotting factor to assist the blood in coagulation when needed.
Treatment classes that increase clotting proteins:
Factor 8 or Factor 9 | Bypassing agents | Factor 8 mimetic | Gene therapy.
Anticoagulant inhibition
Approaches being investigated that aim to block anticoagulant proteins:
Anti-TFPI | APC inhibitor | PS inhibitor | Antithrombin inhibitor.
Some approaches being researched aim to restore balance in a different way. Instead of adding clotting factors they aim to block anticoagulant proteins to help minimize the potential for bleeding.
Approaches being investigated that aim to block anticoagulant proteins:
Anti-TFPI | APC inhibitor | PS inhibitor | Antithrombin inhibitor.
APC=activated protein C; PS=protein S; TFPI=tissue factor pathway inhibitor.
What are treatments that increase clotting proteins?
The following treatments add clotting proteins to assist blood in coagulation when needed:

Factor 8 or Factor 9:
Treatments that replace the clotting proteins that are deficient or defective in patients with Hemophilia A or B.
Bypassing agent:
A product that contains one or more clotting proteins to work around clotting inhibitors.
Factor 8 mimetic:
A substitution treatment that acts as Factor 8 to bridge the clotting cascade.
Gene therapy:
A correction of a gene error by inserting a normal gene to replace an abnormal gene. In hemophilia, a copy of the Factor 8 or Factor 9 gene, whichever is altered, can be inserted into cells.

What are potential strategies being researched that aim to block anticoagulant proteins?
The following potential hemophilia strategies aim to block anticoagulant proteins to help minimize the potential for bleeding:


Anti-TFPI:
Designed to block a protein called tissue factor pathway inhibitor, an anticoagulant protein that inhibits the early phase of the clotting cascade and stops the blood from clotting.
APC inhibitor:
Designed to block a protein called activated protein C, an anticoagulant protein that suppresses clotting by inhibiting Factor 5 and Factor 8.
Protein S inhibitor:
Designed to block Protein S, an anticoagulant acting as a cofactor for APC and TFPI.
Antithrombin inhibitor:
Designed to block a protein called antithrombin, an anticoagulant protein which inhibits the thrombin protein that is needed for blood to clot.
Blood clotting 101: the coagulation cascade
There are two pathways in the coagulation cascade:
The extrinsic pathway (or the tissue factor pathway) is the fast pathway for the start of blood coagulation.
It begins when a blood vessel is injured and the platelets in the wall of the vessel change form as they activate
A protein called tissue factor is exposed to the blood stream and binds to a circulating protein, Factor 7


The intrinsic pathway also plays an important role.
It starts slowly, helping to stabilize the platelet plug and form a clot
It involves circulating proteins in the blood, including Factor 8 and Factor 9
In hemophilia A and B, this pathway is incomplete due to missing or reduced Factor 8 or Factor 9
The common pathway
Once the cascade is started, it leads to the common pathway, where thrombin generation results in the development of a strong, stable fibrin clot that will stop and prevent further bleeding from the vessel into the surrounding tissue.

Different types of administration are being researched
People with hemophilia desire simpler and less burdensome administration they can incorporate into their daily routines.
Prophylaxis therapies are being researched for administration in different methods.
Looking for educational resources?
Our Hemophilia Dictionary defines common terms and concepts to make it easier talk about and understand various bleeding disorders.
Looking for support on your journey?
Find out about advocacy groups, financial support, and resources which may be helpful for you and your family.
Resources for People With Hemophilia
Learn more and stay updated on the latest news about hemophilia research.
Would you like to learn more about research in hemophilia?
Sign up now to receive updates from ChangingHemophilia.com


Discover real hemophilia patient stories
“While I came to terms with the physical implications of my bleeding disorder relatively quickly, it has taken the better part of two decades to reckon with the mental aspects of being a patient.
The bleeding, bruising, and 3 intravenous infusions per week were not the greatest challenges that hemophilia presented. Instead, it was feeling abnormal, fearing that others would treat me differently, and coping with my seemingly unfair reality that occupied most of my headspace.
Years of struggling with these emotions ultimately taught me that we live our lives not despite our most difficult problems, but rather to overcome them and to discover what we are truly capable of. Hemophilia was simply the challenge that life provided me, and it was my desire to use this experience to inform my aspirations, to better understand others, and to find ways to champion my bleeding disorder in the pursuit of serving my community.”
—Garrett lives with severe hemophilia A

Support for people with hemophilia
Where can I find support and community?
When it comes to living well with hemophilia, many people find it beneficial and even essential to spend time with others who have been there too. Get connected with the hemophilia community here.
What is the difference between "patient assistance" and copay programs?
Patient assistance programs support uninsured eligible patients who meet certain requirements with drug costs, while copay assistance programs cover all or part of an uninsured, eligible patient’s out-of-pocket cost for a prescription. In general, patient assistance programs may help supplement insurance coverage for prescribed treatment and copy programs may help cover out-of-pocket costs or prescribe treatment for uninsured patients.
Many manufacturers of hemophilia treatments also offer their own individual programs to offer financial assistance to their patients.
If you are currently receiving treatment for hemophilia, contact the manufacturer of your prescription to find out what kinds of help may be available to you. One way to start would be to search the internet for terms such as "patient assistance" or "co-pay assistance" and the name of your prescription or the company that makes your treatment, if you know it.


Fostering understanding
Our Hemophilia Dictionary defines common terms and concepts to make it easier to talk about and understand various bleeding disorders.
Building community
Get tips on building a strong support system—an important component of living with hemophilia.